
Golfer’s elbow is also known as golfer ‘s elbow, golfer ‘ s elbow or medically epicondylitis medialis humeri.
As with tennis elbow , this is an inflammation of the tendon origin (tendon origin tendinosis). However, in golfer’s elbow, the inside of the elbow joint is affected.
The lower flexor muscles on the inner humeral cartilage, on the little finger side of the elbow joint, are irritated due to occupational or sporting (e.g. golf) overuse. This particularly affects the periosteum.
It is also assumed that chronic cramping of the corresponding muscles plays a significant role in golfer’s elbow. Occasionally, the symptoms are found together with ulnar sulcus syndrome.
In tennis elbow, the outer side of the elbow joint (epicondylus humeri radialis) is affected in a similar way.
Synonyms: Golfer’s elbow, epicondylitis humeri ulnaris, EHU
Anatomy relevant to the golfer’s arm
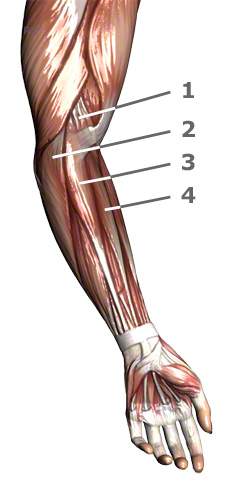
Picture above: Here are the most important muscles that attach to the inner humeral cartilage and are therefore responsible for the golfer’s arm problem: 1, Musculus pronator teres 2, M. flexor carpi ulnaris (only the origin is visible) 3, M. palmaris longus 4, M. flexor carpi radialis
Several forearm muscles, which are jointly responsible for flexing the wrist and fingers, attach to the inner humeral cartilage (epicondylus humeri ulnaris). The symptoms are localized here.
Picture below: X-ray of the elbow: 1, humerus, humerus 2, external cartilage 3, internal cartilage 4, radius, radius 5, ulna, ulna

What complaints are associated with golfer’s elbow?
In golfer’s elbow, overuse of the muscles at their origins triggers a characteristic pain, which can be provoked by pressure on the above-mentioned cartilage or by a typical movement (flexion of the wrist as in a golf swing).
Pain is also described when the forearm is rotated inwards. Functionally, the arm is often enormously restricted. With advanced irritation, a reduction in strength of the corresponding muscles can be seen.
The plastic surgeon must differentiate golf elbow (epicondylitis humeri medialis) from epicondylitis humeri radialis (tennis elbow) and from other diseases.
Wear-related joint changes (osteoarthritis), inflammatory processes and tumors can cause symptoms similar to golfer’s elbow. It is not uncommon for golfer’s elbow to be associated with ulnar sulcus syndrome, which can cause the little finger to tingle.
What options are there for conservative treatment without surgery?
Medicinal treatment for golfer’s elbow includes the application of ointment dressings. Injections of the muscle origins with anti-inflammatory and pain-relieving medication(local anesthetics and cortisone) are also used. In the case of golfer’s elbow, these should certainly be used with more caution due to the proximity of the ulnar nerve. It should not be forgotten that cortisone can lead to nerve damage. If such injections are given repeatedly and possibly directly into the ulnar nerve, permanent damage can be caused which cannot always be repaired by surgery. Finally, wearing an upper arm plaster splint for immobilization or an elbow cuff are further conservative treatment options.
Furthermore, physiotherapy should be tried to stretch and loosen the cramped and possibly shortened forearm flexor muscles.
Picture below: Stretching exercise for golfer’s elbow: With the elbow extended, the wrist is stretched.

What should I know about golfer’s elbow surgery?
If, after approximately six months of conservative treatment, the golfer’s elbow still shows no improvement or even worsens, surgery may be advisable depending on the symptoms. The procedure can be performed on an outpatient basis if there are no reasons (secondary illnesses) for not doing so.
An intravenous regional anesthesia, plexus anesthesia(anesthesia in the armpit) or, in special cases, general anesthesia are possible anesthetic procedures.
Basically, there are two standard procedures available for golfer’s elbow and tennis elbow. The Hohmann operation and the Wilhelm operation. Due to the proximity of the ulnar nerve (ulnar nerve), greater caution is required here.
- Hohmann operation:
In golfer’s elbow, the origins of the muscles that attach here are detached at the inner elbow (humeral cartilage) and further away from the body. - Wilhelm surgery:
Wilhelm surgery involves cutting and obliterating the smallest nerves that supply the inner elbow area. This procedure is also known as denervation. The combination of both procedures is preferred by many surgeons.
In the case of tennis elbow, the operation is performed in a similar way on the thumb side of the elbow.

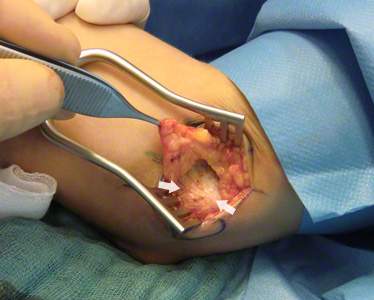
Pictures of the surgery:
1, Typical area of pain radiation from the inner humeral cartilage = circle (epicondylus humeri ulnaris) in the golf elbow. The ulnar nerve runs between the circle and the elbow.
2, Conventional golfer’s arm surgery: right arrow = inner humeral cartilage; left arrow = fibers of the muscle skin (muscle fascia), the originating musculature.
What does minimally invasive surgery mean?
Minimally invasive surgery should be used with caution in the case of golf elbow. The ulnar nerve is located in the immediate vicinity of the surgical site and could be injured if the overview is poor. We therefore do not prefer minimally invasive surgery for golfer’s elbow.
Read also the article Minimally invasive surgery for tennis elbow.
What should I bear in mind after golf elbow surgery?
After the operation, you will wear an upper arm plaster splint for 14 days to immobilize it. Careful movement exercises in the elbow joint can then be started. Depending on the severity of the condition and the healing process, physiotherapy is sometimes useful.
