What are the known causes?
There are many possible causes of carpal tunnel syndrome. The following causes are known:
- Anatomy – Some people have a narrower carpal tunnel than others.
- Injuries – Sometimes even severe strains in the wrist and hand area can cause these complaints.
- Fractures near the wrist
- Recurrent mechanical stress on the wrist (work or sport)
- Inflammation (mostly tendonitis)
- Degenerative changes (age-related signs of wear and tear)
- Tumors(lipoma, ganglion,…) are causes that can lead to carpal tunnel syndrome.
- Rheumatic diseases – Rheumatics often form pronounced changes in the wrist and tend to tendonitis.
- Pregnancy – This is caused by weight gain and water retention.
- Diabetics, dialysis patients and people who are overweight are more frequently affected.
What complaints / symptoms can it be associated with?
In those affected, carpal tunnel syndrome often manifests itself through tingling or numbness in the thumb, index and middle finger during exercise and at night.
Patients often describe it to our team of hand surgeons in Düsseldorf as: Tingling and falling asleep of the hand, hands or fingers, as falling asleep hands or falling asleep fingers.
The symptoms tend to occur in certain positions of the wrist. Patients state that they experience an increase in discomfort when making phone calls, riding a bike or motorcycle, blow-drying their hair and similar movements.
However, the symptoms are also present outside of stressful situations.
How can hand surgeons explain the sometimes severe pain at night?
The sometimes severe nocturnal pain caused by carpal tunnel syndrome can be explained by increased swelling in the carpal tunnel in a lying position and the resulting increased pressure.
Many people also sleep with their wrists bent, narrowing the carpal canal.
Short-term pressure relief can often be achieved simply by shaking the hand.
When the pressure is relieved by an operation at our Yuveo Clinic in Düsseldorf, this pain is quickly reduced. In many cases, it can be almost completely gone by the first night after the procedure.
As our hand surgeons in Düsseldorf will explain to you, the excruciating pain does not always only affect the arm or hand.
The nerve compression can occasionally cause pain to radiate into the shoulder or even the neck.
How do we make the diagnosis at the Yuveo Clinic?
Complaints
In most cases, the symptoms described by our patients in Düsseldorf quickly point to carpal tunnel syndrome. Sometimes, however, the symptoms can be very atypical.
Investigation
It is important to our hand surgeons to examine the sensation of the fingers and the strength of the ball of the thumb. We also examine the entire arm and the other nerves (especially the ulnar nerve) to rule out a combination of other clinical pictures . Is swelling visible in the wrist?
Laboratory and X-ray
A blood test could rule out diabetes mellitus. X-rays show bony changes following fractures or rheumatism (arthritis, polyarthritis, arthrosis).
In the case of carpal tunnel syndrome, we involve the neurologist in Düsseldorf in the diagnosis.
The measurement of the “nerve currents” (= ENG / EMG) by a neurologist (= neurologist) should confirm the suspicion of carpal tunnel syndrome. At the same time, other causes (herniated disc, …) can be ruled out. With the help of this measurement, we can better assess the extent of the damage to the median nerve and the prognosis. It is highly recommended before an operation and should be relatively recent so that we have a reference for the follow-up examinations after the operation.
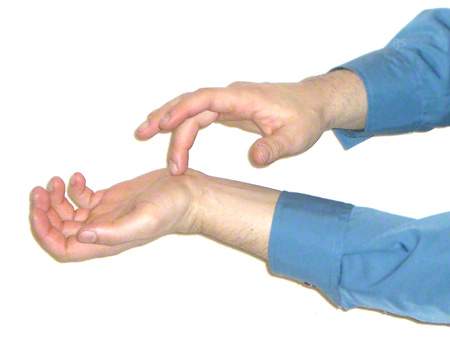
Also: see pictures on the right: the two typical tests to narrow down the symptoms.
How is conservative treatment carried out at our clinic in Düsseldorf?
Carpal tunnel syndrome should initially be treated conservatively before surgery, if the symptoms and the electrophysiological examination by the neurologist allow it.
There are various therapeutic approaches here: Vitamin B6 preparations and non-steroidal anti-inflammatory drugs (NSAIDs) are often prescribed. A night-time positioning splint often also alleviates the symptoms.
Occasionally, unbearable acute attacks of pain may occur, requiring rapid action by the hand surgeon.
In these situations, we can inject a corticoid into the carpal tunnel, which causes a rapid reduction in pain in carpal tunnel syndrome, particularly by inhibiting the swelling of the tendon sheath in the carpal tunnel.
If such injections are given repeatedly and possibly directly into the median nerve, permanent damage can be caused which cannot be repaired by surgery.
What is the follow-up treatment for carpal tunnel syndrome after surgery in Düsseldorf?
 Here you can see a standard stretch-side plastic splint with a wrap, which can be worn for a few days for protection.
Here you can see a standard stretch-side plastic splint with a wrap, which can be worn for a few days for protection.
The majority of our patients experience a significant reduction in pain after the operation. The operation is particularly grateful in view of the often considerable night pain.
This pain often disappears in the first few days, or occasionally in the first night, after the procedure.
In cases of severe damage to the median nerve and usually with a long history of illness, the loss of sensation often does not recover completely. For this reason, surgery should not be postponed unnecessarily.
Depending on the operation and patient activity, wearing a plaster splint for 3-5 days is recommended. However, our plastic surgeons in Düsseldorf advise against wearing the splint for longer, as otherwise there is a risk of the median nerve sticking to the surrounding scar tissue, resulting in corresponding discomfort. The gliding ability of the nerves in the carpal canal is important.
Our hand surgeons recommend gentle, non-strenuous movement exercises as early as three days after the operation. Physiotherapy is very important for advanced diseases with muscle atrophy.
We remove the stitches after approx. two weeks at the Yuveo Clinic. We recommend a neurological-electrophysiological check-up after about 3-6 months if the postoperative course is normal.